Laparoscopic Herniorrhaphy
Hernia Repair
Hernia:
A hernia is a weakness in the abdominal wall resulting in abnormal protrusion of abdominal contents (e.g. intestines) through the defect. Hernias enlarge over time and may become incarcerated (fail to reduce) or strangulated (loss of hernia contents due to lack of blood supply). A hernia should be surgically repaired. Although most hernias occur in the groin (eighty-percent), they may also be located in the navel, upper-inner thigh, and along previous abdominal incisions.
Symptoms:
Increased abdominal pressures caused by lifting heavy objects, coughing, substantial weight gain, or straining with bowel movements and the like may call a patients attention to a hernia.
Symptoms may include:
- Abnormal bulge
- Pain or tenderness
- Abdominal distention
- Failure to pass flatus
- Constipation
- Diarrhea
- Fevers or chills
- Nausea and vomiting
Diagnosis:
History and physical are the most useful tools in the diagnosis of a hernia. If clinical uncertainty persists after examination, an ultrasound or CT may provide your doctor with information showing bowel protruding through an abdominal wall defect.
Surgery:
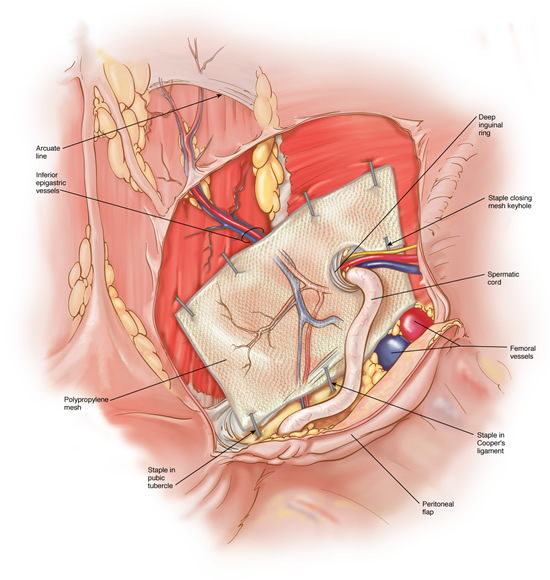
Laparoscopic hernia repair may be considered in nearly all patients diagnosed with an abdominal wall hernia. Laparoscopic repair involves quarter-inch incisions through which a camera and instruments are placed. Open hernia repair requires a 3-5 inch incision. The abdominal wall defect is repaired with mesh and secured under direct vision of the laparoscope. Patients with hernias in both groin may be repaired through the same incisions.
Recovery:
Patients recover sooner after laparoscopic hernia repair. Return to activities can occur within 2-3 days compared to 2-4 weeks with an open approach. Pain experienced by the open technique is greater and longer lasting. Wound infections occur less frequently with the laparoscopic technique.
Pertinent References
Frantzides, C.T., Welle S., Laparoscopic Repair of Complex Scrotal Hernia. Video Atlas of Advanced Minimally Invasive Surgery, Sounders Elsevier 2013
Frantzides, CT, Madan A, Carlson M; Laparoscopic Diaphragmatic Hernia Repair, Not Involving the Hiatus; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Frantzides, CT, Carlson M; Laparoscopic Incisional-Ventral Hernia Repair; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Frantzides, CT, Zografakis J Carlson M; Laparoscopic Transabdominal Inguinal Hernia Repair; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Carlson MA, Frantzides, C.T., Shostrom MS, Laguna LE; A Review of 6,266 Published Cases of Minimally Invasive Ventral Herniorrhaphy: An Analysis of 6,266 Cases. Hernia. 12: 9-22, 2008.
Frantzides, C.T., Madan AK, Zografakis JG, Smith C: Laparoscopic Repair of Incarcerated Diaphragmatic Hernia. J Laparoendosc. Adv. Surg. Tech. 17: 39-42, 2007.
Frantzides, C.T., Carlson MA; Technical Factor Predisposing To Recurrence After Minimally Invasive Incisional Herniorrhaphy; Recurrent Herniation. V Schumpelick and RJ Fitzgibbons (ed.). Springer. 170-178, 2007.
Frantzides, C.T., Carlson MA, Zografakis JG, Madan AK, Moore RE; Minimally Invasive Incisional Herniorrhaphy: A Review of 208 Cases; Surgical Endoscopy 18: 1488-1491, 2004
Frantzides, C.T., Madan AK, O’Leary PJ, Losurdo J. Laparoscopic Repair of a Recurrent ChronicTraumatic Diaphragmatic Hernia; American Surgeon 69(2):160-162, 2003
Carlson MA, Richards CG, and Frantzides CT: Laparoscopic prosthetic reinforcement of hiatal herniorrhaphy. Dig Surg 16:407-410, 1999.
Frantzides CT, Carlson MA: Prosthetic reinforcement of posterior cruroplasty during laparoscopic hiatal herniorrhaphy. Surg Endosc 11: 769-771, 1997.
Frantzides CT, Carlson, MA: Minimally invasive ventral herniorrhaphy. J. Laparoendosc Surg. 7:121-124, 1997.