Laparoscopic Diaphragmatic Hernia Repair
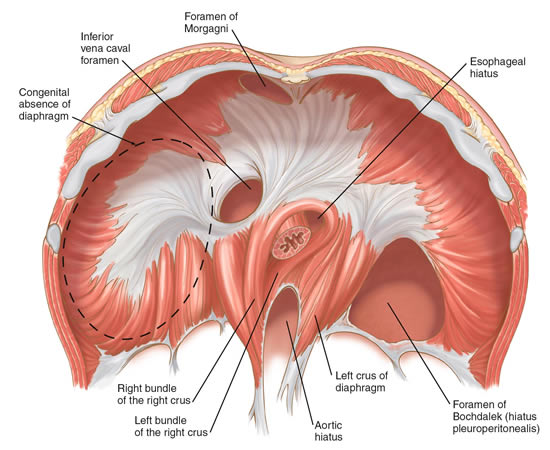
A. The Condition. The diaphragm is the muscular wall which separates the contents of your chest from your abdomen. The diaphragm helps you take breaths. A hernia of the diaphragm is a weakened area, essentially a hole, through which contents of the abdomen (such as intestines) can push through and into the chest. This can cause pain, difficulty breathing, and severe infection in rare cases.
B. Symptoms
- Chest pain
- Crampy pain abdominal pain
- Shortness of breath
- Gurgling in the chest
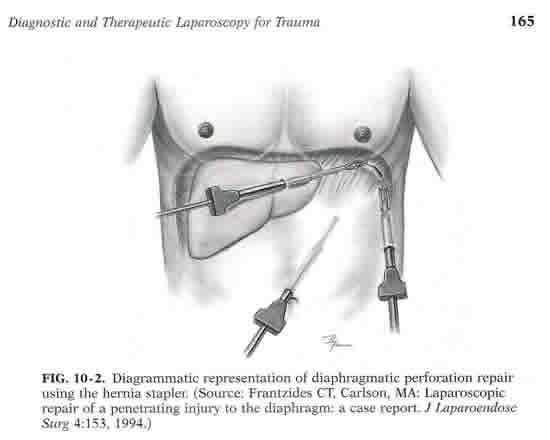
C. Laparoscopic Diaphragmatic Hernia Repair. The surgeon will make about 3-4 small incisions in your abdomen. A port (nozzle) is inserted into one of the slits, and carbon dioxide gas inflates the abdomen. This process allows the surgeon to see inside of your abdomen more easily. A laparoscope is inserted through another port. The laparoscope looks like a telescope with a light and camera on the end so the surgeon can see inside the abdomen. Surgical instruments are placed in the other small openings and used to repair the diaphragmatic hernia. This type of hernia usually is repaired by placing a soft plastic mesh over the hole (the hernia), and stapling this mesh to the surrounding diaphragm edge. After this has been accomplished, the carbon dioxide is released out of the abdomen through the slits, and then these sites are closed with sutures or staples, or covered with glue-like bandage and steri-strips.
Dr. Frantzides was the first ever to perform a Laparoscopic repair of penetrating injury to the diaphragm in 1994 and Laparoscopic repair of a Congenital Diaphragmatic Hernia in 2000.
D. Nonsurgical Treatment. There is really no other treatment other than surgery for this problem.
E. Risks. The primary risks of laparoscopic diaphragmatic hernia repair are:
Infection of the skin at one of the small ports sites
Pneumothorax (a collection of air in the chest which may need to relieved with a tube)
Postoperative ileus (the intestines slow down/stop working for several days)
Injury to the intestine
F. Expectations
1. Before Your Operation. Laparoscopic diaphragmatic hernia repair usually is an elective procedure. The preoperative evaluation might include blood work, urinalysis, barium swallow x-ray, and a CT scan. If you smoke, then you should stop immediately. If you are taking blood thinners (for example, aspirin, coumadin, Lovenox, or Plavix), then you will need to stop these one week prior to your procedure. Your surgeon and anesthesia provider will review your health history, medications (including blood thinners), and options for pain control.
2. Your Recovery. You usually can go home in 1 or 2 days after a laparoscopic diaphragmatic hernia repair. You will be given medication for pain. You should limit your activity to light lifting (no more than 15 lb) for one month.
3. Call Your Surgeon if you have one or more of the following:
- Severe pain
- High fever
- Difficulty breathing or swallowing
- Odor or increased drainage from your incision
- No bowel movements for three days
G. Pertinent References
Frantzides CT, Carlson MA. Laparoscopic repair of a penetrating injury to the diaphragm: a case report. J Laparoendosc Surg. 1994;4(2):153-6.
Frantzides CT, Carlson MA, Pappas C, Gatsoulis N. Laparoscopic repair of a congenital
diaphragmatic hernia in an adult. J Laparoendosc Adv Surg Tech A. 2000 Oct;10(5):287-90.
Frantzides CT, Madan AK, O’Leary PJ, Losurdo J. Laparoscopic repair of a recurrent chronic
traumatic diaphragmatic hernia. Am Surg. 2003 Feb;69(2):160-2.
Carlson MA, Frantzides CT. “Mesh-Reinforced Repair of Diaphragmatic Hernia.” In: Schumpelick V, Nyhus LM, eds. Meshes: Benefits and Risks. Berlin: Springer, 2004.
Frantzides CT, Madan AK, Zografakis J, Smith C. Laparoscopic repair of incarcerated diaphragmatic hernia with mesh. J Laparoendosc Adv Surg Tech A. 2007 Feb;17(1):39-42.
Frantzides CT, Madan AK, Carlson MA. “Laparoscopic Repair of Diaphragmatic Hernia Not
Involving the Hiatus.” In: Frantzides CT, Carlson MA, eds. Atlas of Minimally Invasive Surgery.Philadelphia: Saunders Elsevier, 2009.
Ayiomamitis. G.D, Avramidou.A., Tsavolakis. T.,Kouroumpas. E., Frantzides C.T. “Huge Chronic Trauma Rapture of the Left Diaphragm Complicated with Massive Visceral Herniation and Colon Obstruction: Laparoscopic Primary Suture Repair, Spearing the Chest Tube” J Laparoendosc. Adv. Surg.Tech. Videoscopy January 2013