Minimally Invasive Esophagectomy (removal of esophagus)
A. The Condition. You may have a tumor or cancer of your esophagus. If the tumor has not spread beyond the esophagus, then usually the best treatment is to remove the esophagus.
B. Symptoms
- Difficulty swallowing
- Weight loss
- Heartburn (this can be present for years)
- Spitting up
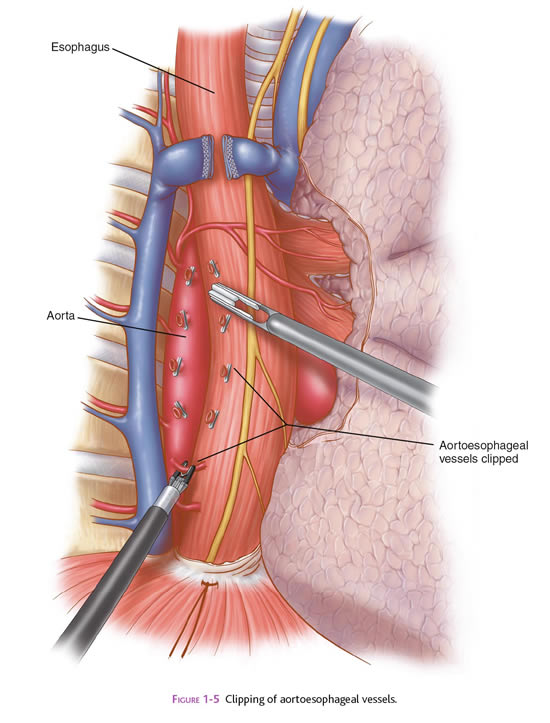
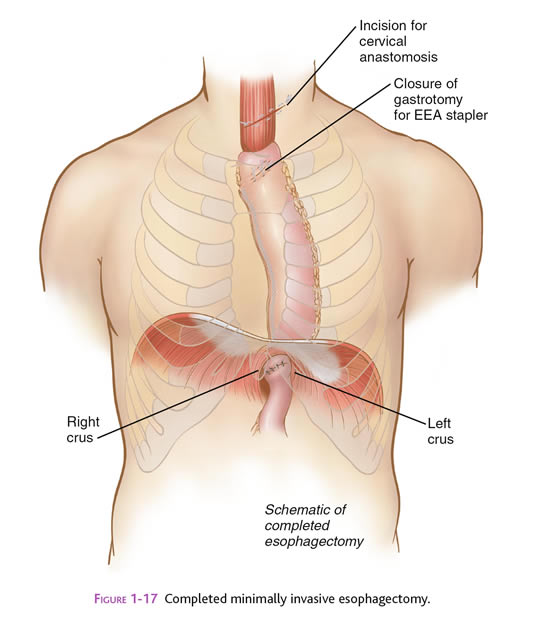
C. Minimally Invasive Esophagectomy. This procedure typically is done by operating in both the chest and abdomen. Your surgeon will discuss with you the best approach for your situation. One common approach is to free up the esophagus by inserting ports (nozzles) into the chest for passage of a laparoscope and surgical instruments. The laparoscope looks like a telescope with a light and camera on the end so the surgeon can see inside the abdomen. The thoracic surgeon will insert a laparoscope and instruments into your chest, and free up the esophagus. After the esophagus is free within the chest, the stomach is freed up by inserting the ports in the abdomen. Your stomach then will be pulled into your chest to serve as a replacement organ for your esophagus, so that you will be able to eat and drink normally. You also may have an incision in your neck where your surgeon will connect the stomach (which has been pulled up from the abdomen) to the remnant of the esophagus. After all this has been accomplished, the surgical sites are closed with sutures or staples, or covered with glue-like bandage and steri-strips. When you wake up, You may also have some temporary tubes in place: (1) a feeding tube (pencil-thin) in your small bowel, which comes out of the left side of your abdomen; and (2) a chest tube, which comes out of the side of your right or left chest.
D. Nonsurgical Treatment. Sometimes your doctors may recommend that your tumor is treated with radiation and chemotherapy before having surgery. If you have a esophageal tumor that has spread beyond the esophagus, then surgery to remove the esophagus usually is not indicated. Your doctors will discuss your treatment options with you if this is the case.
E. Risks. Esophagectomy can be a very difficult operation for the patient, and there are many risks. The primary risks of minimally invasive esophagectomy are:
- Heart attack
- Heart rhythm abnormality
- Pneumonia
- Leakage of the connection between the stomach and the esophageal remnant
- Dying off of the stomach
- Internal bleeding
- Infection of the skin at one of the small ports sites
- Postoperative ileus (the intestines slow down/stop working for several days)
- Death (up to 5% of cases, depending on your state of health before surgery)
F. Expectations
1. Before Your Operation. Minimally invasive esophagectomy is usually an elective procedure. The preoperative evaluation might include blood work, urinalysis, abdominal x-rays, upper endoscopy (looking into your esophagus from the throat with a scope), and an abdominal CT scan. You also may have a barium x-ray of your esophagus. If you smoke, then you should stop immediately. If you are taking blood thinners (for example, aspirin, coumadin, Lovenox, or Plavix), then you will need to stop these one week prior to your procedure. You may need an extensive evaluation of your heart and lungs to determine if you are fit for surgery. Your surgeon and anesthesia provider will review your health history, medications (including blood thinners), and options for pain control.
2. Your Recovery. You usually can go home in 5-7 days after a minimally invasive esophagectomy. You may have to wait for your bowels to start working. Your may have to adjust your diet to eat smaller, more frequent meals. You will be given medication for pain, and you may be given antibiotic pills. You should limit your activity to light lifting (no more than 15 lb) for one month.
3. Call Your Surgeon if you have one or more of the following:
- Severe chest or abdominal pain
- High fever
- Odor or increased drainage from your incision
- No bowel movements for three days
G. Pertinent References.
Kent M, Luketich JD. “Minimally Invasive Esophagectomy.” In: Frantzides CT, Carlson MA, eds. Atlas of Minimally Invasive Surgery. Philadelphia: Saunders Elsevier, 2009.