Laparoscopic Esophagomyotomy (Heller Myotomy)
Division of Lower Esophageal Muscle
Achalasia:
Achalasia is a motility disorder of the esophagus. It is characterized by lack of the normal wave-like motion of the esophagus and lack of relaxation of the lower most portion of the esophagus. Degeneration of the nerves in the wall of the esophagus, that control this function, is known to be the cause of this disorder. The cause of the degeneration is unknown.
Symptoms:
The symptoms associated with achalasia are consistent and include:
- Swallowing difficulty
- Regurgitation (undigested food)
- Chest pain
- Respiratory symptoms (undigested food into the airway)
Diagnosis:
Several studies are helpful to your doctor in making the diagnosis of achalasia.
X-ray:
- Dilated esophagus
- Fluid within the esophagus
- Enlarged esophagus
- Tapering (“Bird’s Beak”) esophagus
- Outpouching (diverticulum) of the lower esophagus
Endoscopy:
- Rule-out cancer
- Degree of inflammation
Manometry:
- Increased pressure at the lower esophagus
- Failure of lower esophagus to relax
- Failure of wave-like motion of the esophagus
Surgery:
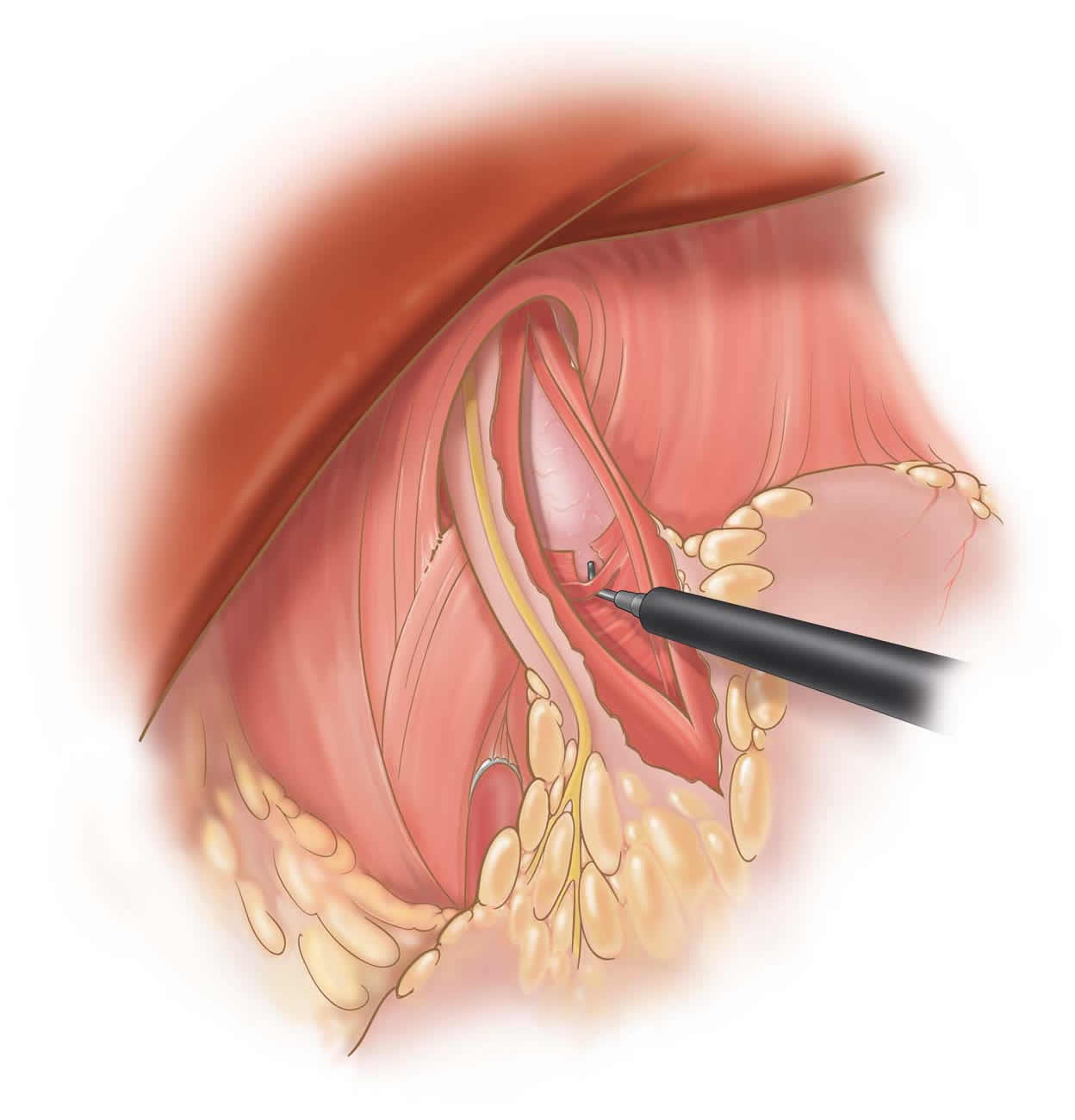
Laparoscopic esophagomyotomy is superior to all other forms of treatment for achalasia. Balloon dilatation, botulism toxin injection, and medical management with calcium channel blockers fail to completely and permanently resolve symptoms. Traditional surgical approaches involve either a 6-8 inch incision in the left chest or a 6-8 inch incision in the upper abdomen. The laparoscopic approach involves making five quarter-inch incisions on the abdomen through which a camera and four instruments are placed. The esophageal muscle is incised with a specially insulated laparoscopic instrument. A portion of the upper stomach is then wrapped around the lower portion of the esophagus to prevent reflux. Patients are discharged the first post-operative day after a swallow study is obtained.
Dr. Frantzides techniques and clinical outcomes of the laparoscopic procedure were published in 2004. This is one of the largest series on laparoscopic esophagomyotomy in the world.
Recovery:
Patients recover sooner after laparoscopic esophagomyotomy. Return to activities can occur within 3-7 days compared to 4-6 weeks with an open or thoracoscopic approach. Wound infections occur less frequently with the laparoscopic technique. Also, less pain has been reported with laparoscopy.
Pertinent References
Frantzides, C. T., Luu M., Laparoscopic esophagomyotomy. Video Atlas of Advanced Minimally Invasive Surgery, Sounders Elsevier pp 49-53; 2013
Frantzides, C.T., Moore RE, Madan AK Carlson MA, Keshavarzain A, Smith C; Achalasia:
Minimally Invasive Surgical Approach: A 10 Year Experience. J. Gastrointestinal Surg. 8:18-23, 2004
Frantzides CT, Carlson MA: Minimally invasive surgery of the esophagus. Proceedings of the 15th World Congress of Collegium Internationale Chirurgiae Digestivae, J.P. Kim and R.E. Condon Ed. Monduzzi Editore, Bologna, Italy, pp. 27-31-1996.