Laparoscopic Fundoplication
Gastroesophageal Reflux Surgery
Gastroesophageal Reflux:
Gastroesophageal reflux disease (GERD) occurs when the esophagus is exposed to prolonged periods of stomach acid. A defective lower esophageal sphincter is responsible for most cases of reflux. The lower esophageal sphincter (LES) is a high pressure zone near the junction of the stomach and esophagus. Normally the LES acts like a valve closing after swallowing. The LES fails to close adequately in patients suffering with GERD allowing the esophagus to be exposed to acid. Heartburn, esophagitis, esophageal stricture, and even cancer may result from GERD.
Symptoms:
The symptoms associated with GERD are variable but generally include:
- Heartburn – 30 – 60 minutes after eating
- Regurgitation – worsened with lying flat
- Excessive belching
- Aspiration – stomach contents refluxed into the airway
- Asthma – chronic result of aspiration
- Chest pain – burning mid-chest pain
- Difficulty swallowing
- Pain with swallowing
- Bleeding
Diagnosis:
Several studies are helpful to your doctor in making the diagnosis of hiatal hernia including:
Esophagram:
Assess the function of the esophagus
Identify structural abnormalities (esophageal stricture)
Reveal associated problems (e.g. aspiration, poor gastric emptying)
Upper endoscopy:
Identify damage caused by reflux (e.g. Esophagitis, Barrett’s esophagus, malignancy)
Biopsy esophagus for evaluation of malignancy
Esophageal manometry:
Assess the function of the LES
Assess the wave-like motion (propulsive function) of the esophagus
Surgery:
Laparoscopic Nissen fundoplication is a viable option after failure of lifestyle changes, sufficient attempts at medical management, or prolonged medical management. Lifestyle changes typically include:
- Weight loss
- Smoking cessation
- Reduced fatty food intake
- Reduced consumption of caffeinated and carbonated beverages
- Elevation of the head of the bed during sleeping
- No oral intake four to six hours prior to going to sleep
Medical management may include:
- Over-the-counter antacids
- H2 blockers (stomach acid production blockers)
- Proton pump inhibitors (stomach acid production blockers)
- Stomach motility agents (quicker stomach emptying and increase LES pressure)
- Stomach lining coating agents (protects healing portions of the stomach)
- (While the treatments listed above may resolve symptoms, patients will continue to have gastroesophageal reflux)
Surgical Management:
In the past, surgery was a last resort because of the prolonged recovery time and large painful incision involved with the procedure. With the new minimally invasive approach, surgery is now a viable option after early attempts of modifications and medical management fail to adequately resolve symptoms.
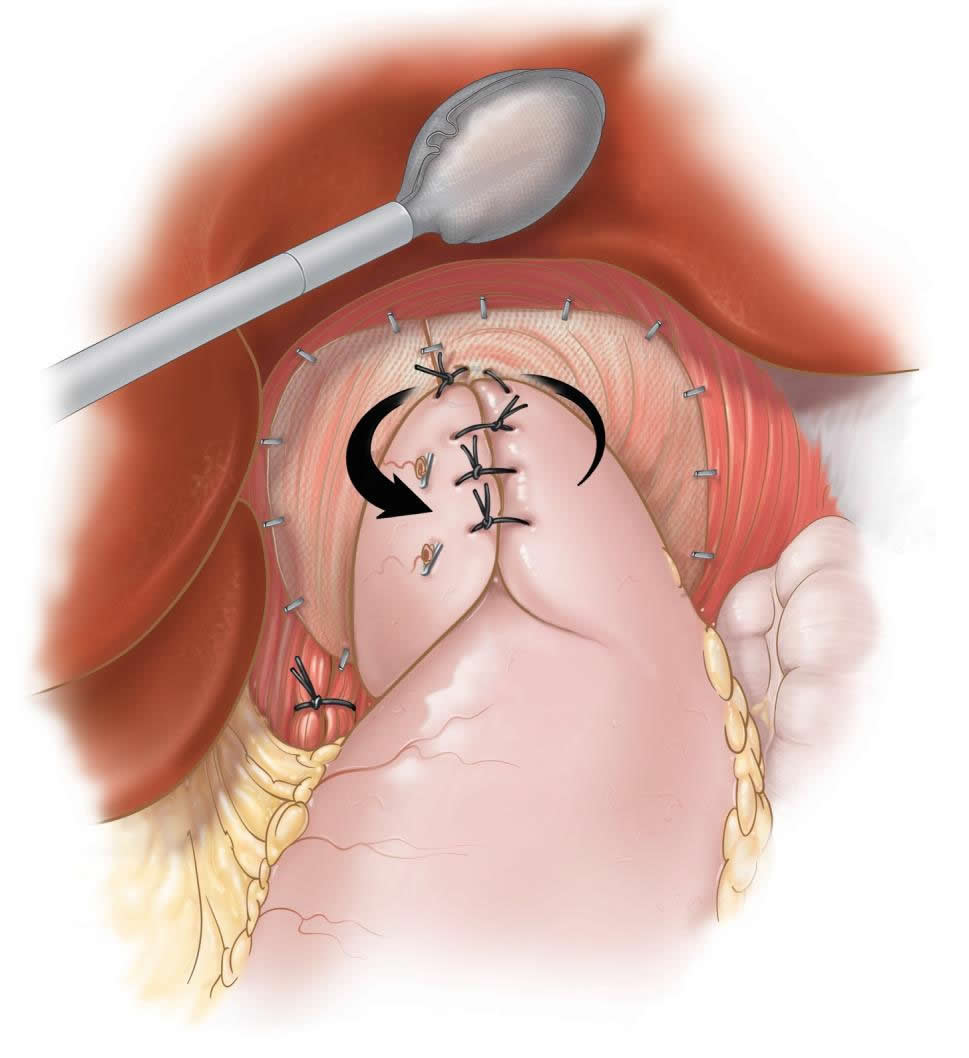
The laparoscopic Nissen fundoplication is performed through five quarter-inch incisions through which, a camera and four instruments are placed. A new lower esophageal valve is constructed by wrapping a two-centimeter portion of the stomach around the lower most portion of the esophagus. This collar is then anchored to the tough fibers of the diaphragm (the respiratory muscle separating the chest from the abdomen). The procedure typically lasts for forty-five minutes to one and a half hours. Patients are started on clear liquids the next morning and are discharged in the afternoon. The open surgical technique involves an 8-10 inch upper abdominal incision with a hospital stay of 5-7 days.
Dr. Frantzides has published extensively on the technical aspects of the laparoscopic fundoplication and introduced “The Frantzides Algorithm” for the preoperative evaluation of patients with gastro-esophageal reflux disease (G.E.R.D.).
Recovery:
Patients recover sooner after laparoscopic Nissen fundoplication. Return to activities can occur within 2-7 days compared to 4-6 weeks with an open approach. Wound infections occur less frequently with the laparoscopic technique. Also, less pain has been reported with laparoscopy. Most importantly, greater than ninety-percent of patients are symptom free ten years after the procedure.
Pertinent References
Frantzides, CT, and Carlson, MA: Laparoscopic VS. Conventional Fundoplication. J. Laparoendosc Surg. 5(3):137-143, 1995.
Frantzides CT, Carlson MA: Laparoscopic re-do Nissen fundoplication. J. Laparoendosc Surg., 7: 235-239, 1997.
Frantzides CT, and Richards CG: A study of 362 consecutive laparoscopic Nissen fundoplications. Surgery 124(4):651-654, 1998.
Frantzides CT, Carlson, MA: Minimally invasive Nissen fundoplication with hernia repair. Hellenic Laparosc. Surg. 2:12-19, 1999.
Carlson MA, Frantzides C.T.: Complications and Results of Laparoscopic Antireflux Procedures: A Review of 10,489 Cases. J. Am. Coll. Surg. 193:428-439, 2001
Frantzides, C.T., Madan AK, Carlson MA, Stewart ET, Smoth C; Selective use of Esophageal Manometry Monitoring Prior to Laparoscopic Fundoplication: J. Am Coll. Surg 197(3) 358-364. 2003
Frantzides, C.T., Madan AK, Moore RE, Zografakis JG, Carlson MA, Keshavarzian A: Laparoscopic Esophageal Mucosal Resection for High-Grade Dysplasia; J. Laparoendosc. Advanced Surg. Techniques 14(5) 261-265, 2004.
Granderath FA, Frantzides, C.T., Carson MA; Hiatal Closure—New Trends in Laparoscopic Antireflux Surgery; Gastroesophageal Reflux Disease: Principles of Disease, Diagnosis and Treatment. FA Granderath, T kamolz, R Pointer (ed.). Vienna: SpringerWien New York, 2006.
Granderath FA, Carlson MA, Champion JK, Szold A, Basso N, Frantzides, C.T.: Prosthetic Closure of the Esophageal Hiatus in Large Hiatal Hernia Repair and Laparoscopic Antireflux Surgery; Surgical Endos
Frantzides, C.T., Carlson MA, Zografakis JG, Moore RE, Zeni TM, Madan AK: Postoperative Complaints After Laparoscopic Nissen Fundoplication; J Soc Laparoendosc. Surg; 10: 39-42, 2006.
Frantzides, CT, Carlson M; Laparoscopic Fundoplication; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Frantzides, C.T., Madan AK,Carlson MA, Zeni TM, Zografakis JG, Moore RE, Meiselman M, Luu M, Ayiomamitis G; Laparoscopic Revision of Failed Fundoplication and Hiatal Herniorrhaphy. J. Laparosc. Adv. Surg. Tech. 19(2): 133-139, 2009
Frantzides, C.T., Carlson M.A.; Welle. S. Minimally Invasive Surgical Therapy for Gastrointestinal Reflux Disease and Hiatal Hernia; In Textbook of General Surgery, Ed; Sayek I, p1960, 2012