Laparoscopic Drainage of Pancreatic Pseudocyst
A. The Condition. A pseudocyst is an abnormal fluid-filled cavity within the pancreas. Pseudocysts usually are a consequence of severe inflammation of the pancreas (pancreatitis). Pseudocysts can cause internal bleeding and/or infection, so surgical removal often is indicated.
B. Symptoms
- Nausea, vomiting
- Fevers, chills
- Jaundice
- Abdominal pain
- Weight loss, weakness
- Abdominal mass
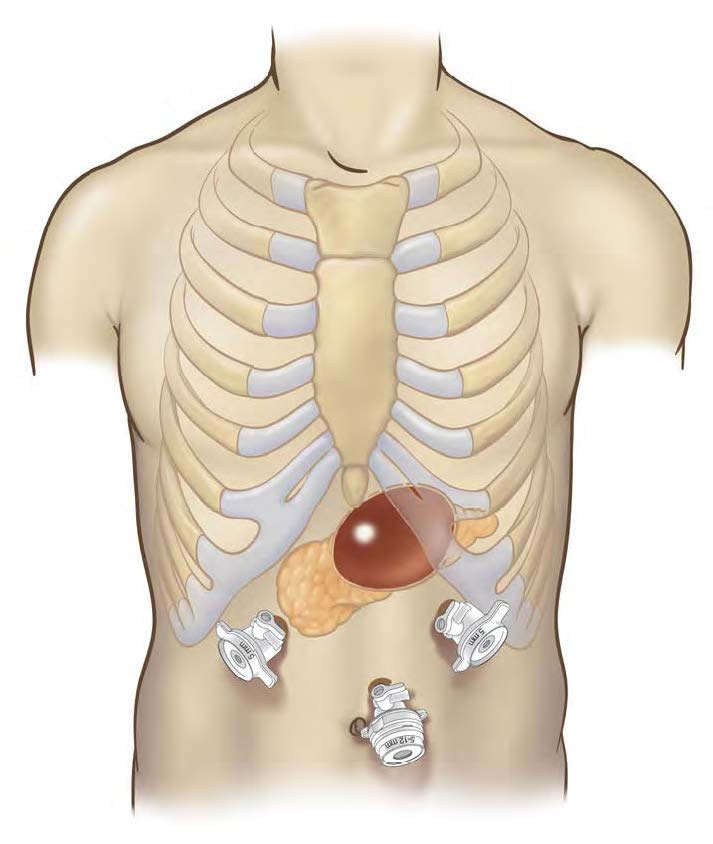
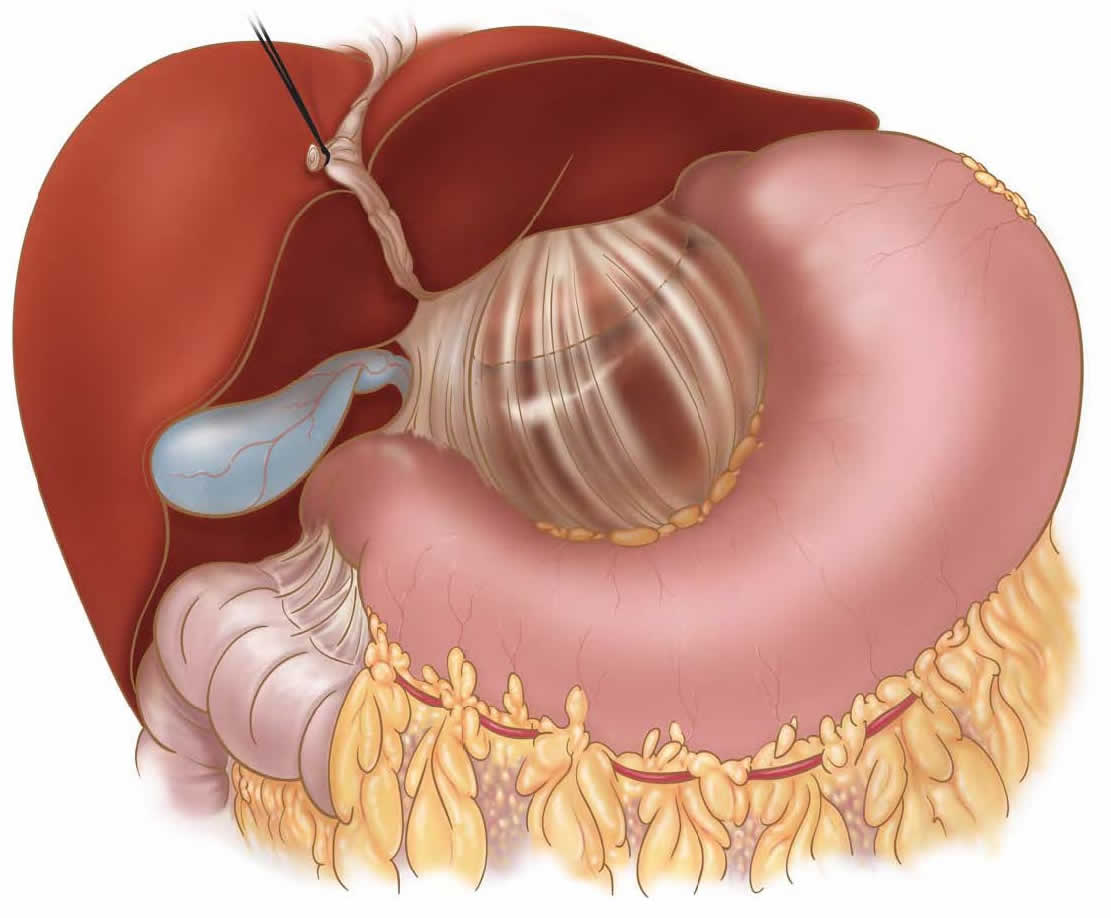
C. Laparoscopic Drainage of Pancreatic Pseudocyst. The surgeon will make about 4-5 small incisions in your abdomen. A port (nozzle) is inserted into one of the slits, and carbon dioxide gas inflates the abdomen. This process allows the surgeon to see inside of your abdomen more easily. A laparoscope is inserted through another port. The laparoscope looks like a telescope with a light and camera on the end so the surgeon can see inside the abdomen. Surgical instruments are placed in the other small openings and used to perform the drainage procedure. Typically, the pseudocyst is drained into the stomach or small bowel. This is done with surgical staplers. Sometimes a small rubber drain is placed, and this exits the skin from your abdomen. After this has been accomplished, the carbon dioxide is released out of the abdomen through the slits, and then these sites are closed with sutures or staples, or covered with glue-like bandage and steri-strips.
The first in the world Laparoscopic Drainage of Pancreatic Pseudocyst was performed by Dr. Frantzides in 1993 and was reported in 1994.
D. Nonsurgical Treatment. Sometimes your problem may be treated with a catheter that the radiologist can insert through your skin. Your doctor will discuss with you what your best option is.
E. Risks. The primary risks of laparoscopic drainage of pancreatic pseudocyst are:
- Infection of the skin at one of the small ports sites
- Leakage of pancreatic juice at the surgical site
- Collection of pus inside your abdomen (intraabdominal abscess)
- Postoperative ileus (the intestines slow down/stop working for several days)
- Internal bleeding
- Small bowel obstruction (kinking of the small bowel, causing blockage)
F. Expectations
1. Before Your Operation. Laparoscopic drainage of pancreatic pseudocyst usually is an elective procedure. The preoperative evaluation might include blood work, urinalysis, endoscopy (looking down your throat with a scope), an abdominal CT scan, and perhaps a x-ray of your biliary tract with dye. If you smoke or drink, then you should stop all of this immediately. If you are taking blood thinners (for example, aspirin, coumadin, Lovenox, or Plavix), then you will need to stop these one week prior to your procedure. Your surgeon and anesthesia provider will review your health history, medications (including blood thinners), and options for pain control.
2. Your Recovery. You usually can go home in 2-5 days after a laparoscopic drainage of pancreatic pseudocyst. You may need to wait until your bowels start working. You will be given medication for pain, and you may be given antibiotic pills. If you have a drain in place, then your doctor and/or nurse will instruct you in its care. You should limit your activity to light lifting (no more than 15 lb) for one month.
3. Call Your Surgeon if you have one or more of the following:
- High fever
- Severe abdominal pain
- Odor or increased drainage from your incision
- Jaundice
- No bowel movements for three days
- Vomiting blood, or blood in your stool
G. Pertinent References
Frantzides, CT, Ludwig, K., Redlich, P. Laparoscopic Management of Pancreatic Pseudocyst. J.Laparoendosc. Surg. 4:55-59, 1994.
Bilimoria MM, Frantzides CT, Laguna LE. “Minimally Invasive Distal Pancreatectomy.” In: Frantzides CT, Carlson MA, eds. Atlas of Minimally Invasive Surgery. Philadelphia: Saunders Elsevier, 2009.