Laparoscopic Gastrectomy (resection of stomach)
A. The Condition. You may have a tumor of your stomach which needs to be removed by surgery. The precise location of the tumor will determine how much (all or some) of your stomach that will need to be removed. Your doctors will discuss this with you.
B. Symptoms
- Nausea, vomiting
- Abdominal pain
- Weight loss, weakness
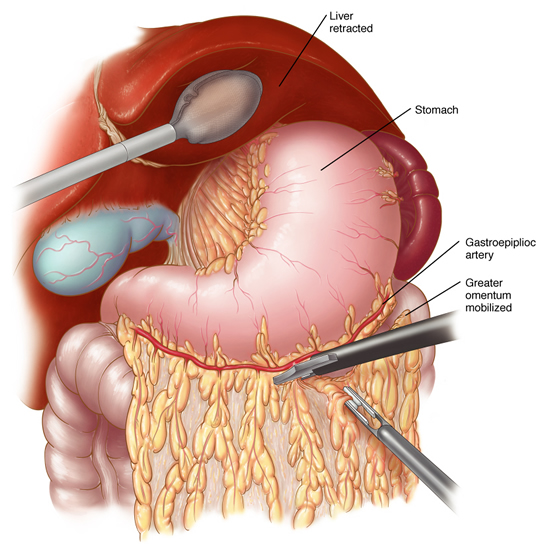
C. Laparoscopic Gastrectomy. The surgeon will make about 4-5 small incisions in your abdomen. A port (nozzle) is inserted into one of the slits, and carbon dioxide gas inflates the abdomen. This process allows the surgeon to see inside of your abdomen more easily. A laparoscope is inserted through another port. The laparoscope looks like a telescope with a light and camera on the end so the surgeon can see inside the abdomen. Surgical instruments are placed in the other small openings and used to remove the portion of the stomach that contains the tumor. The stomach specimen is removed in a plastic bag from the abdomen by enlarging one of the small incisions on your abdomen. After all or some of stomach has been removed, your small intestine will be connected to the esophagus or remnant of the stomach, so that you will be able to eat again. This connection is done with surgical staplers. After this has been accomplished, the carbon dioxide is released out of the abdomen through the slits, and then these sites are closed with sutures or staples, or covered with glue-like bandage and steri-strips.
D. Nonsurgical Treatment. Chemotherapy for stomach tumors is generally not effective, so surgery usually is the best option for a tumor that is localized to the stomach. If the tumor has spread beyond the stomach, then your doctor will discuss your treatment options with you.
E. Risks. The primary risks of laparoscopic gastrectomy are:
- Infection of the skin at one of the small ports sites
- Leakage of the connection between the stomach and small bowel
- Collection of pus inside your abdomen (intraabdominal abscess)
- Postoperative ileus (the intestines slow down/stop working for several days)
- Small bowel obstruction (kinking of the small bowel, causing blockage)
- Pneumonia
F. Expectations
1. Before Your Operation. Laparoscopic gastrectomy usually is an elective procedure. The preoperative evaluation might include blood work, urinalysis, a barium swallow x-ray, endoscopy (looking down your throat with a scope), an abdominal CT scan, and perhaps a nuclear medicine scan. If you smoke and/or drink, then you should stop immediately. If you are taking blood thinners (for example, aspirin, coumadin, Lovenox, or Plavix), then you will need to stop these one week prior to your procedure. Your surgeon and anesthesia provider will review your health history, medications (including blood thinners), and options for pain control.
2. Your Recovery. You usually can go home in 3-4 days after a laparoscopic gastrectomy. You may need to wait until your bowels start working. You will be given medication for pain. You should limit your activity to light lifting (no more than 15 lb) for one month.
3. Call Your Surgeon if you have one or more of the following:
- High fever
- Severe abdominal pain
- Odor or increased drainage from your incision
- No bowel movements for three days
G. Pertinent References
Madan AK, Frantzides, C.T., Keshavarzian A, Smith C; Laparoscopic wedge resection of gastric leiomyoma; J. Soc. Laparoendosc. Sur. 8:77-80, 2004
Frantzides CT, Zografakis JG. “Laparoscopic Bypass with Roux-en-Y Gastrojejunostomy.” In: Frantzides CT, Carlson MA, eds. Atlas of Minimally Invasive Surgery. Philadelphia: Saunders Elsevier, 2009.
Parikh M, Pomp A. “Laparoscopic Total Gastrectomy For Malignancy.” In: Frantzides CT, Carlson MA, eds. Atlas of Minimally Invasive Surgery. Philadelphia: Saunders Elsevier, 2009.