Minimally Invasive (Laparoscopic) Ventral Hernia Repair
A. The Condition. A hernia is a weakness or defect in the muscles and tissues of your abdominal wall. The contents of your abdomen (such as intestines) can push through a hernia, causing a bulge and discomfort. Ventral hernias involve the front of your abdomen, and commonly occur at the site of a previous surgical incision. Groin hernias are covered in another brochure. A ventral hernia can be repaired by covering the defect with a piece of soft plastic mesh.
B. Symptoms
- Bulge in your abdominal wall
- Abdominal pain
- Change in bowel habits
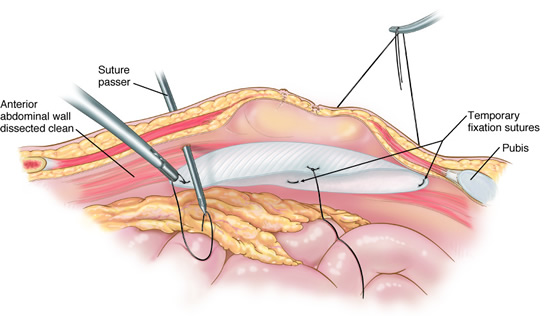
C. Minimally Invasive Ventral Hernia Repair. The surgeon will make about 3-4 small incisions in your abdomen. A port (nozzle) is inserted into one of the slits, and carbon dioxide gas inflates the abdomen. This process allows the surgeon to see inside of your abdomen more easily. A laparoscope is inserted through another port. The laparoscope looks like a telescope with a light and camera on the end so the surgeon can see inside the abdomen. Surgical instruments are placed in the other small openings and used to repair the ventral hernia. Your surgeon first will have to remove all the intestines which may have become entrapped into the hernia. This process by itself can be very difficult and time-consuming. After the intestines have been removed from the hernia, the repair usually is done by placing a soft plastic mesh over the hole (the hernia), and stapling this mesh to the surrounding edge of the abdominal wall. If you have a large hernia, then you may require a very large sheet of mesh, more than 12 inches across. After this has been accomplished, the carbon dioxide is released out of the abdomen through the slits, and then these sites are closed with sutures or staples, or covered with glue-like bandage and steri-strips.
Dr. Frantzides was the first to describe a Laparoscopic Incisional Hernia Repair with “dual layer prosthesis” in 1997. In 2004 he published one of the largest series of Laparoscopic Ventral (incisional) Hernia Repairs.
D. Nonsurgical Treatment. There is really no other treatment other than surgery for this problem. If you have a small ventral hernia that is not causing you symptoms, then you and your doctor may decide not to perform surgery on it.
E. Risks. The primary risks of minimally invasive ventral hernia repair are:
- Infection of the skin at one of the small ports sites
- Postoperative ileus (the intestines slow down/stop working for several days)
- Injury to the intestine
- Infection of the mesh
F. Expectations
1. Before Your Operation. Minimally invasive ventral hernia repair usually is an elective procedure. The preoperative evaluation might include blood work, urinalysis, and possibly a CT scan. If you smoke, then you should stop immediately. If you are taking blood thinners (for example, aspirin, coumadin, Lovenox, or Plavix), then you will need to stop these one week prior to your procedure. Your surgeon and anesthesia provider will review your health history, medications (including blood thinners), and options for pain control.
2. Your Recovery. You usually can go home in 1 or 2 days after a minimally invasive ventral hernia repair. You will be given medication for pain. You should limit your activity to light lifting (no more than 15 lb) for at least one month. Your surgeon may want to limit your activity for a longer period, depending on how complex your repair was.
3. Call Your Surgeon if you have one or more of the following:
- Severe pain
- High fever
- Abdominal pain
- Odor or increased drainage from your incision
- No bowel movements for three days
G. Pertinent References
Frantzides CT, Carlson MA. Minimally invasive ventral herniorrhaphy. J Laparoendosc Adv Surg Tech A. 1997 Apr;7(2):117-20.
Frantzides CT, Carlson MA, Zografakis JG, Madan AK, Moore RE. Minimally invasive incisional herniorrhaphy: a review of 208 cases. Surg Endosc. 2004 Oct;18(10):1488-91.
Frantzides, C.T., Carlson MA; Technical Factor Predisposing To Recurrence After Minimally Invasive Incisional Herniorrhaphy; Recurrent Herniation. V Schumpelick and RJ Fitzgibbons (ed.). Springer. 170-178, 2007.
Carlson MA, Frantzides CT, Shostrom VK, Laguna LE. Minimally invasive ventral herniorrhaphy: an analysis of 6,266 published cases. Hernia. 2008 Feb;12(1):9-22.
Frantzides CT, Carlson MA, Zografakis JG. “Laparoscopic Ventral Hernia Repair.” In: Frantzides CT, Carlson MA, eds. Atlas of Minimally Invasive Surgery. Philadelphia: Saunders Elsevier, 2009.
Frantzides, C.T., Roberts, J.,Zeni T., Welle S.; Laparoscopic mesh repair of Parastomal hernia. Video Atlas of Advanced Minimally Invasive Surgery, Sounders Elsevier pp 263-265;2013
Frantzides, C.T., Welle, S., Laparoscopic Reduction of Internal Hernia, Video Atlas of Advanced Minimally Invasive Surgery, Sounders Elsevier 2013